Kidney cancer is among the 10 most commonly diagnosed cancers in both men and women. Through the use of radiographic imaging and needle biopsies, urologists at Weill Cornell Medicine can evaluate your unique situation to help you choose from the best treatment options. We offer minimally invasive and robotic-assisted surgeries, as well as thermal ablation therapies and chemotherapy.
In 2015, about 61,560 new cases of kidney cancer (38,270 in men and 23,290 in women) were diagnosed, and approximately 14,080 people (9,070 men and 5,010 women) died from it.
Kidney cancer is among the 10 most commonly diagnosed cancers in men and women, respectively.
The average age of people when they are diagnosed is 64 years. Kidney cancer is very uncommon in people younger than age 45 years.
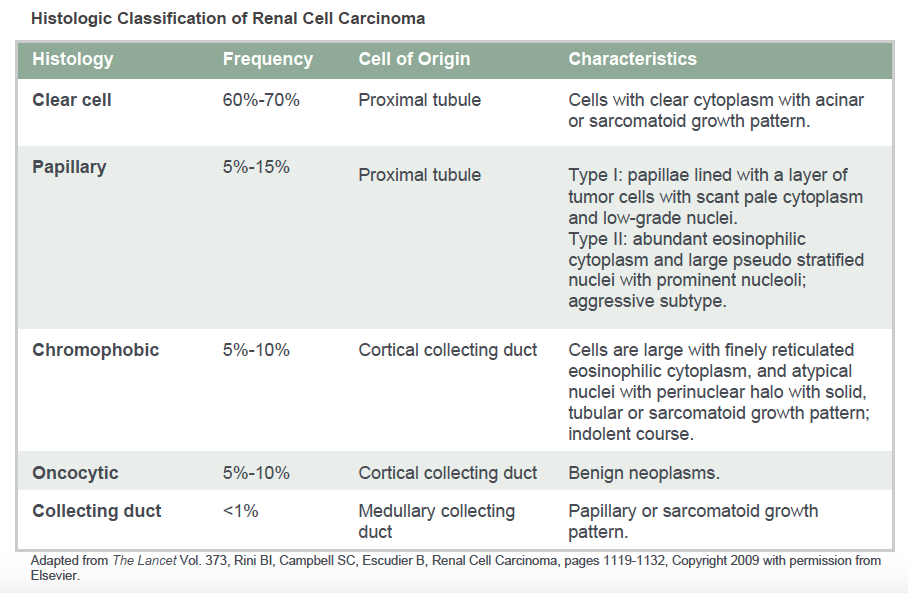
Kidney Cancer Histology: (see chart below)
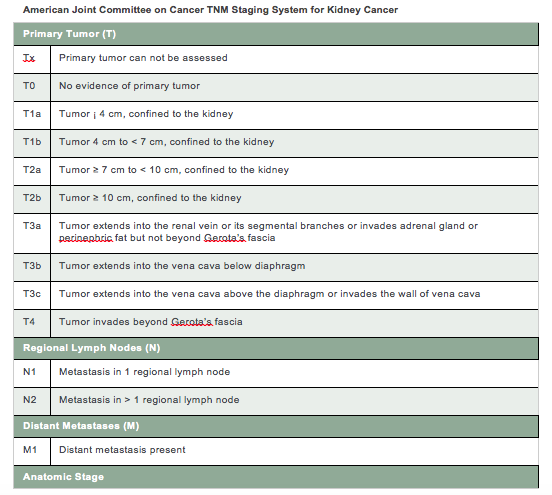
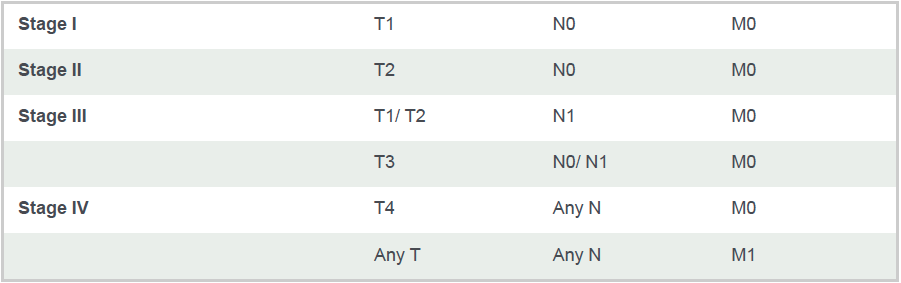
The 5 year overall survival rate for kidney cancer by stage from the National Cancer Database is below. Overall survival accounts for death due to other causes, such as heart disease.
Kidney cancers are also assigned a Furhman Grade of 1 through 4.
- Grade 1 cancers have cell nuclei that are similar to normal kidney cell nuclei. These cancers usually grow and spread slowly and tend to have a favorable prognosis.
- Conversely, grade 4 cancer nuclei appear very different from normal kidney cell nuclei, and have an unfavorable prognosis.
Risks & Causes
The lifetime risk for kidney cancer is approximately 1 in 63 (1.6%), and the risk is approximately 2-3 times higher in men than in women.
Other risk factors include obesity, smoking, exposure to industrial agents containing cadmium, hypertension, dialysis for kidney failure and a family history of kidney cancer.
Inherited kidney cancers comprise just 5% of all kidney cancers.
von Hippel-Lindau syndrome
- A mutation in the VHL gene leads to a greater risk for developing renal cell carcinoma, especially at an earlier age.
- There is also risk for benign tumors in the eyes, brain, spinal cord, pancreas and other organs.
- In addition, there is a greater risk for pheochromocytoma, a type of adrenal gland tumor.
Hereditary papillary renal cell carcinoma
- A mutation in the MET gene is associated with papillary renal cell carcinoma.
Hereditary leiomyoma-renal cell carcinoma
- Mutations in the FH gene are associated with smooth muscle tumors (fibroids) of the skin and uterus in women, and an increased risk for papillary renal cell carcinoma.
Birt-Hogg-Dube (BHD) syndrome
- Mutations of the FLCN gene is associated with benign kidney tumors (oncocytoma) and renal cell carcinoma.
- In addition, it is associated with skin tumors, particularly on the face, neck, and upper chest and cysts in the lungs.
Symptoms & Evaluation
In the past, kidney cancers were diagnosed only after they had grown significantly in size, leading to symptoms of flank pain, blood in the urine, or palpable mass in the abdomen.
Other symptoms include weight loss, fevers, persistent fatigue and swelling in the lower extremities.
With greater use of radiographic imaging such as ultrasound, CAT scan or MRI, most kidney cancers are now found incidentally (during evaluation of unrelated medical problems) by imaging studies.
A needle biopsy may be performed under image guidance in the case of small renal masses (<4 cm in diameter), as up to 30% of kidney masses of this size may not be cancerous. This is usually performed as an outpatient procedure and the risk of spreading kidney cancer along the needle tract is about 1 in 1000, and the risk of bleeding is very low.
Compete evaluation includes imaging of the chest, lungs and abdominal organs and lymph node to determine whether the cancer has spread beyond the kidney.
Treatment Options
Surgery
- Under general anesthesia, radical nephrectomy or complete removal of the kidney and fat around the kidney is performed when it is not possible to perform a partial nephrectomy, or to just remove the cancerous portion of the kidney. This is often performed through a minimally invasive/laparoscopic approach which requires an overnight hospital stay except with larger renal masses, in which an open surgical incision may be required.
- Because the other kidney has normal function in most individuals, there are usually no functional consequences. However, whenever possible, a partial nephrectomy is performed to maximize kidney function.
- In comparison with a radical nephrectomy, a partial nephrectomy is associated with a higher risk of bleeding, requiring blood transfusion and urine leak as a consequence of wedging out the cancerous portion of the kidney. Robotic-assisted partial nephrectomy via a minimally invasive approach is used for renal masses generally up to 7 cm depending on surgeon experience, and open partial nephrectomy is performed for larger masses.
- With both partial and radical nephrectomy, the kidney cancer is removed, allowing the pathologist to examine the tissue and determine the pathologic stage. This allows additional prognosis, or prediction in terms of recurrence-free survival.
Thermal Ablation
- Heat (radioablation) or cold (cryotherapy) may be used to kill the kidney cancer with image guidance, typically under general anesthesia.
- Several probes are inserted through the skin and abdominal wall muscles.
- With this approach, the mass is not removed, but rather left in place.
- Population-based studies demonstrate that more imaging was performed after thermal ablation compared to surgical removal of kidney cancers.
Chemotherapy
- For cancer that has spread beyond the kidney, chemotherapies include:
- Sunitinib
- Sorafenib
- Pazopanib
- Axitinib
- Temsirolimus
- Everolimus
- Bevacizumab in combination with interferon
Would you like an appointment?
To request an appointment, please call our office at (646) 962-6363. Our phone staff are available to help you Monday-Friday, from 9AM-5PM (EST).
If you'd like to learn more about our providers that specialize in Kidney Cancer, please view the "Our Care Team" page.